History
The typical incubation period from exposure to development of symptoms is 4 days but can range from 1-26 days. Prodromal symptoms of local pain, tingling, itching, and burning often precede development of the rash. Constitutional symptoms of fever, fatigue, myalgias, and headache often accompany the primary herpes simplex virus (HSV) infection.
Herpetic lesions usually begin as clusters of small bumps, then blisters, followed by open sores or ulcers. Lesions coalesce and usually heal over several weeks at various rates.
Many times these classically described lesions in the genital area may not present in all patients and may be difficult to differentiate from other conditions such as syphilis and chancroid.
Local pain is a prominent and common complaint. Patients with genital herpes may also complain of pain in the groin area secondary to local adenopathy. Women often present with complaints of genital swelling, discharge, and dysuria.
Many primary infections are asymptomatic. Up to 63% of women with HSV-2 antibodies have no clinical history of infection. [10] 87.4% of 14-49 year olds have never received a diagnosis despite being infected [11] . However, when primary infections are symptomatic, they are usually more severe than recurrent infections. Persons with asymptomatic genital HSV-2 infections still shed virus but less frequently than persons with symptomatic infections. [12]
Recurrent lesions are common and typically occur during periods of stress.
-
Patients may give a history that includes the following:
Occupational exposure
Herpetic whitlow, found in health care workers (especially medical or dental)
Herpes gladiatorum on bodies of wrestlers
Previous history of herpetic diseases
-
Immune status
Malnourishment
Hematological malignancies
Bone marrow transplant
Renal transplant
Cardiac transplant
-
Neurologic symptoms
Headache
Confusion
Fever
-
Lesions
Location varies
May be very painful
Tenesmus, itching with anal/perianal lesions
Dysuria and/or discharge with genital lesions
Sore throat with oral lesions
-
Prodromal symptoms (present in advance of herpes lesions)
Burning
Itching
Tingling
Pain
-
Constitutional symptoms (usually present with development of herpes lesions)
Anorexia
General malaise
Fever
Headache
Myalgias
Physical
Physical examination findings of HSV vary depending on location of the lesions.

General findings
-
Lesions usually are vesicular or ulcerative on an erythematous base, as shown in the image above.
-
Lesions coalesce and then heal over the next several weeks.
-
Tender bilateral lymphadenopathy occurs with genital lesions.
Skin infections (HSV-1 or HSV-2)
-
Herpetic whitlow or paronychia on the fingers of healthcare workers (not to be confused with abscess). This usually is due to infection with HSV-1, but HSV-2 infections may be seen with digital-genital contact.
-
Herpes gladiatorum on the bodies of wrestlers and other sports that involve close physical contact. It has been estimated that in Division I National Collegiate Athletic Association (NCAA) wrestling, the incidence of herpes gladiatorum can be as high as 20-40%.
Oropharyngeal disease
-
Gingivostomatitis (herpes labialis on the lips, shown in the image below)
-
Submandibular lymphadenopathy
-
Fever

Genital herpes
-
Painful vesicular or ulcerative lesions may appear similar to chancroid or syphilis (vesicular lesions shown in the image below)
-
Inguinal lymphadenopathy
-
Genital lesions, especially urethral lesions, may cause transient urinary retention in women
-
Vaginal discharge

Keratoconjunctivitis
-
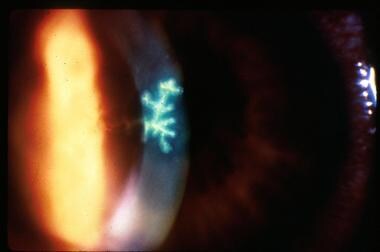
Dendritic keratitis found with slit lamp (dendritic ulcer shown in the image below)
-
Corneal ulcers
-
Vesicles on eyelids
Neurologic
-
New psychiatric symptoms (indicative of encephalitis) - Confusion; seizures; meningeal signs (Recurrent lymphocytic meningitis [benign form of meningitis/encephalitis that may occur during primary HSV-2 infection])
-
Bell palsy (possible relationship with HSV-1)
Anal/perianal involvement
-
Discharge
-
Vesicles
-
Ulcerations
-
Inguinal adenopathy
Causes
Transmission occurs via contact with the virus through herpes lesions, mucosal surfaces, and genital or oral secretions. [13]
HSV-1 is transmitted through direct contact with infected saliva or direct contact with contaminated utensils.
HSV-2 usually is acquired as an STD.
The maternal-fetal transmission risk for transmission is greater during primary outbreak (30-50%) than with recurrent outbreaks (< 1%). [7]
Recurrent disease (reactivation) is due to certain stimuli: fever, physical or emotional stress, ultraviolet light exposure, or axonal injury.
Complications
Encephalitis: Rare complication of herpetic infection; commonly HSV-1 (hypothesized to spread to the brain via neural routes after primary or recurrent infection)
Neonatal infections: Range from mild localized infection to a fatal disseminated disease; HSV-2 is usually spread via the maternal genital tract; congenital infections possible
Compromised host: Progressive and disseminated disease possible
Genital infection: Acute urinary retention
-
Cutaneous vesicles characteristic of herpes simplex virus infection.
-
Herpes labialis.
-
Penile infection with herpes simplex virus type 2.
-
Tzanck smear showing a multinucleated giant cell.
-
Herpes simplex virus dendritic ulcer with fluorescein staining.
-
Genital herpes infection.








